
– Satchit Balsari, HSPH Kumbh Mela Team Leader
*With apologies to Professor Eck 🙂
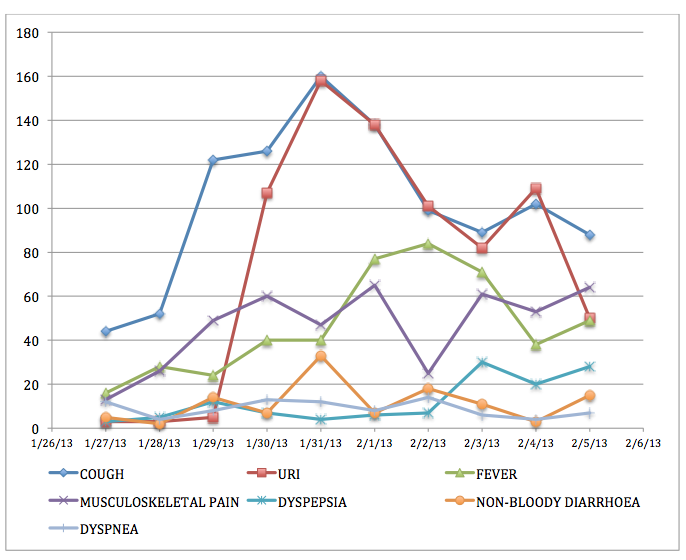
Yesterday, our team crossed the 30,000 mark. Since January 27th, 2013, the four sector hospitals that we have been following have seen over 30,000 patients. The hospital in Sector 11 has seen four times as many patients as that in sector 4. Upper respiratory complaints continue to dominate the presentation to the clinics (about 32%), with fever and musculoskeletal pain close behind. Over 58% of the medications dispensed were analgesics (pain medications) and a quarter were anti-histamines, all of which are available over the counter, without requiring the presence of a physician.

FXB/EMcounter Team consolidating a long day’s work
As we have repeatedly said on this blog, the political will and commitment to making the Mela a success is unprecedented, yet the staggering crowds that come to the Mela repeatedly overwhelm the system: the 30-120 second window for doctor-patient interaction, as the current data reveals, is far from the ideal that the Mela authorities had aspired to.
The size of this data set will allow the authorities to examine several seminal issues surrounding healthcare delivery: prescription practice, resource allocation, epidemiology, and patient behavior at the sector hospitals in the Mela. Our analysis will hopefully influence planning and resource allocation for future Melas. Furthermore, having successfully demonstrated that it is indeed possible to collect such large quantities of data in this chaotic environment, we hope to work with the National Disaster Management Authority of India to consider piloting digital data collection in future mass gatherings in India.
As Dhruv points out, “quality data fosters accountability.” And quality data will help local authorities explore a whole range of new possibilities: engaging more mid-level providers and junior practitioners to see the large volume of patients, reserving the physicians’ time for the more acute cases; piloting cleaner cooking measures, educating the pilgrims on clean water, sanitation, hygiene.
Soon we will bring our surveillance at the sector hospitals to a close, but before we do that, we wanted to share the story of our team with you: the story of 20 public health and medical students from Allahabad and Mumbai who, armed with a handful of iPads, two mobile hotspots, five broken rental bikes, one portion innovation, two portions gumption, and a diehard commitment, logged over 1800 hours of work in 20 days to help this team achieve its goals.
The tool we used to log data is called “EMcounter” – it was originally developed by emergency residents at NewYork-Presbyterian Hospital (NYP) in 2006 to “count” the medical emergencies that presented to casualty wards of hospitals in India that were moving away from traditional one room receiving rooms to more sophisticated emergency departments staffed by trained emergency physicians. After its initial successful run at Sundaram Medical Foundation in Chennai, in 2007, EMcounter stayed dormant for a few years until a mobile tablet-based version was tested in South Sudan in 2012. EMcounter now had the capacity to collect data off-line on mobile devices, and could also analyze raw data in real time, as soon as it was uploaded. In other words, we needed several iPads to digitize the records at the sector hospitals, and mobile hotspots to guarantee generous internet availability to the data collectors. Both easily acquirable. Indian companies rent iPads, and mobile hotspots are an inexpensive investment.
What we needed was the official nod to collect this data, and an army of field staff to digitize the patient records. The National Disaster Management Authority of India provided the former and good Kumbh Mela karma the latter. Namita introduced us to Nutan Maurya, who had already been working with the other Harvard teams. As early as December, Nutan had lined up students from Allahabad’s Sam Higginbottom Institute of Agriculture Technology and Sciences. The Agriculture Institute (as it was formerly known) offers India’s oldest two-year Masters in Public Health. Senior specialists from NDMA, Naghma Firdaus, helped us identify a contact person in the Allahabad Medical College – Dr. Shraddha Dwivedi, also superintendent of Allahabad’s largest public hospital, Swaroop Rani Nehra Hospital. Dr. Shraddha Dwivedi who extended this team her enthusiastic and whole hearted support, made available a steady stream of rotating medical interns to augment this team.

Sam Higginbottom Public Health Team

The local team and Aaron Heerboth.
Initially we wanted to cover all 10 sector hospitals and build some redundancy into the staffing. We were looking for more field researchers. Like our Allahabad group, future team members needed to be familiar with medical jargon, the public sector healthcare system, bilingual, and at ease negotiating the potential morass of bureaucratic red tape and obstructionism they may encounter. By then we had already made several trips back and forth between various authorities all of whom supported the project and all of whom were unable to provide us the requisite permission, until the NDMA stepped in.
Over serendipitous chai in the home of a loving Parsi family in South Mumbai, in an old house overlooking Marline Lines and Saifi Hospital, during a sort-of reunion of the Rotaract Club of the Caduceus, five medical students from Maharashtra thought it worth their while to commit their time and resources to spend two weeks at the Kumbh Mela in Allahabad. The Rotaract Club of the Caduceus, of which I was also once a member, was started in 1997 as a non-governmental organization committed to community service. What started as a motely group of 15 medical students is now a bustling organization of over 120, that conducts cataract camps, large fund-raising drives, and sometimes launches a nation-wide campaign to recruit student volunteers to conduct research in the world’s largest gathering. Panjak Jethwani and Ahmed Shaikh assembled two impressive teams of medical students from Mumbai, Nagpur and Allahabad, after vetting applications from across India and Nepal.
Our team was now almost ready. There was one missing ingredient. Aaron Heerboth.
India Today has written about Aaron’s exercise routine at the Mela and German television has done a segment on Aaron given instructions to the local team. Aaron is a graduating medical student from Weill Cornell Medical College. He is now almost a Kalpavasi! He is certainly the Harvard Kumbh Mela Team’s longest resident member at the Nagri. Having arrived with the initial team in January, by the time the second public health team reached the Mela in early February, Aaron had consolidated his daily routine at the Mela: it involved running long distance between the sector hospitals, dodging cows, crowd and sadhus, jumping over grey water ditches and steering his moped away from the slushy mud that collects at the edges of the metal plates lining the roads.
By February we had realized that the large numbers of patients presenting at the clinics everyday would make it impossible for us to cover all ten clinics. We simply did not have the manpower to do that. We chose instead to pick four representative hospitals based on their diversity of location, accessibility and patient volume. Teams of two, three or sometimes four field staff were required to collect data at these centers. And every day, the overworked Mela physicians had to be gently reminded the importance of documenting at least the chief complaint and the medication dispensed. That was the limit of the medical chart. To expect anything more was foolhardy – given the few seconds that the physicians had per patient encounter it was no surprise that more could not be recorded. Interpreting handwriting, chasing down missing registers, drawing vertical columns in the ledger books and motivating the field researchers every day, sometimes several times a day constituted Aaron’s morning routine.

Patient Registers before transcription to EMcounter.
Here are excerpts from Aaron’s notes to us:
“After somewhat clumsily navigating Allahabad’s shared rickshaw system this morning (which involved several transfers and numerous price negotiations) and a good 3 KM run through crowds of Sadhus, I arrived on site at sector 4 just after 9am to meet our eager public health students.
It appears that today we continue to be (somewhat) reliably up and running with Kumbh Mela EMcounter! Through numerous polite discussions, we have resolved some major physician handwriting issues at sectors 4 and 13, and our four public health students stationed at those hospitals are not having any significant problems. However, one team of two people with one iPad seems somewhat inadequate for sector 4 if we don’t want to overburden our data collectors. Sector 4, however, is on the main road to the Sangam, and has been seeing about 700 patients per day. Hopefully with thearrival of the Mumbai reinforcements, we can have more iPads andpeople at this site. I also think that at all sites, a larger show of presence will help motivate the physicians to document better records.

Local medical students talk with project leader Aaron Heerboth.
The local team and Aaron Heerboth.
At 10:30 I had another Sadhu-dodging run to meet up with the medical interns covering sites X and Y. Things also appear to be going quite smoothly there. Unfortunately, at sector X the physicians are refusing to record chief complaint/diagnosis. I spoke to the physician in charge and tried to explain the big picture importance of recording this data (and I also mentioned that his superiors request it), and he seems to understand, but we will see where this goes.
Logistics summary for today:
Sector 11: Approximately 300 patients, all recorded. Started out with two iPads and 4 people and finished entering the 300 patients in about two hours.
Sector 13: Approximately 350 patients, half recorded wanted them to start fresh today but this was a miscommunication. They should be able to cover all patients from now on. I do feel bad because I very rarely make it to that site given that it’s about 4 km from the others. I did run there once today to thank the physicians for working well with our team.”
Aaron’s run through the Mela starting assuming legendary proportions – a news article mentioned it, bloggers blogged about it, and a satirical piece even disparaged it. Another few weeks and Aaron would soon become the “Running Baba.”
Aaron reported on the Mumbai team’s arrival: “Today was our first day in the field with the new Mumbai students as well as our first day with a fresh batch of Allahabad students. The Mumbai students were actually able to rent a rickshaw for the day and visit each site with me. They were not enthused about my proposed running method. Our rickshaw tour helped orient them to the very disorienting Kumbh area, and they also assisted with several hundred patient entries at the busy sectors 11 and 12. The dust and poor roads seemed to get the best of a couple of them, but overall they are very excited to be on board.”
Ahmed’s diary:
“It’s been 24 hours of alot of travel and dust. We started off from Lucknow in the train, only an hour late. Great journey. Kind of gave us the idea of the general infrastructure and health conditions that we were heading into. Allahabad at 10pm and 9°C. The owners of the place picked us up as they promised earlier, although I don’t remember them mentioning they’re gonna be drunk while they do it. The place is fabulous. Great rooms. Great bathrooms. But….. No water heater. Every time we touch water, it’s like the limb might fall off. Luckily I carried a heating coil, the services of which I’m offering to my team members in return for rent free stay over these fifteen days. The matter is under negotiations. Aaron was super nice to come by and meet us late night just after we arrived. It was great to get oriented the night itself. We downloaded the EMcounter application and had a short demo of how it’s used . He’s made a great network of people who help him get around places. Not that he needs them to do it.
Next morning:
We hired a 6 seater rickshaw for Aaron to show us around the entire Kumbh site and the medical facilities. The medical facilities are great. They’ve got great inpatient wards, some would say, even better than the ones we have in established tertiary care hospitals.
This is how we work:
The doctors are required to keep a record of all patients and medicines administered. This register, has poorly recorded data. We borrow the register from the day before and feed it into the application. We are in the process of getting a signed and stamped letter from the highest health authority of the Kumbh.”

The rickshaws didn’t last long. Boys will be boys. And soon, the team had rented a few scooters that they used to navigate the crowds and cows and Mahavir, Jagdish and Triveni Roads up and down the Kumbh Mela. Little by little, our fantastic team of students from across India were learning the principle of public health field research: tenacity, ingenuity, patience, persistence, improvisation, and innovation.
We left a week ago, but the project continues. This week the team met Rishi Madhok, another emergency physician from NYP, and the technical lead for EMcounter, who arrived in Allahabad a newly married man, straight from his honeymoon. Rishi will work with the local team to expand the survey to the Central Hospital in Sector 2 where we will capture a wholly different set of pathologies – sicker patients with more complex medical problems presented to the Central Hospital.

Ghanshyam and Raunak learning to prepare serial dilutions.
We will remember our time at the Kumbh Mela fondly. The chanting, the smells, the music emanating from every street. The dense crowds on Mauni Amavasya. The millions that stood in waist deep waters and raised their palms to the sun as millions before them always have. It was spectacular. It was poetic. And it was profoundly humbling.
But interacting with our local team was equally, if not more, exhilarating. Reading Avnish’s policy recommendations for future Melas, following Abhishek on a tour of his hospital wards, listening to Aditi oscillate between psychiatry and pulmonology as her career choice, supporting Ahmed as he worried about the incoming team-mates that cancelled their tickets after the stampede, observing Aaron navigate his way around the Mela like he was strolling on the lower east side of Manhattan, and watching Ghanshyam engrossed over a tuberculin syringe dripping E.coli contaminated water onto a culture plate, we were reminded of our collective pursuit of knowledge — unfettered by age, gender, caste or creed.
At the world’s largest gathering of faith, we had bonded over science.

[…] EMcounting the Mela: From Chennai to Prayag (FXB Center Blog, February 20, 2013) […]